Clinical supervision documentation is critical for meeting licensing requirements, ensuring accountability, and protecting both supervisors and supervisees legally. Without proper records, supervisees risk losing credit for hours worked, and supervisors may face legal risks. Here’s what you need to know:
- Supervision Ratios: Many states, like West Virginia, require a 20:1 ratio (1 hour of supervision for every 20 hours of client work). Falling short can cost supervisees up to 33% of their clinical hours.
- What to Document: Include session date, duration, modality, attendees, case discussions (using client initials for privacy), feedback, and ethical challenges.
- Formats: Use frameworks like SOAP, DAP, or BIRP to organize notes systematically.
- Signatures & Storage: Both supervisor and supervisee must sign notes, which should be securely stored (encrypted systems or locked cabinets) for at least seven years.
- Legal Compliance: State licensing boards and organizations like NBCC have strict documentation standards. Missing or incorrect records can invalidate hours.
Supervision Documentation Made Simple
sbb-itb-ce1c1e8
What to Include in Supervision Notes
Clinical Supervision Note-Taking Frameworks: SOAP vs DAP vs BIRP
Supervision notes are more than just a formality – they’re essential for meeting licensing board requirements and ensuring legal and professional accountability. Leaving out crucial details could risk your clinical hours or create potential legal issues.
Required Information for Each Session
Start with the basics: include the session date (MM/DD/YYYY), start and end times, duration, and modality (e.g., in-person or telehealth). List everyone present and, if relevant, the session number.
When documenting client cases, use initials or ID codes instead of full names to stay HIPAA-compliant. Include key details such as diagnostic considerations, interventions discussed, and the supervisee’s response to feedback. For example, you might write: "Discussed client J.M., age 34, presenting with PTSD symptoms. Reviewed trauma-focused CBT. Supervisee will apply grounding techniques and report on outcomes."
Make sure to note any ethical challenges or complex scenarios ("gray areas") brought up during the session. These records demonstrate adherence to professional standards and provide a reference if questions arise later. Also, reflect on the supervisee’s strengths, areas needing improvement, and conversations about countertransference or self-care strategies.
How to Structure Your Notes
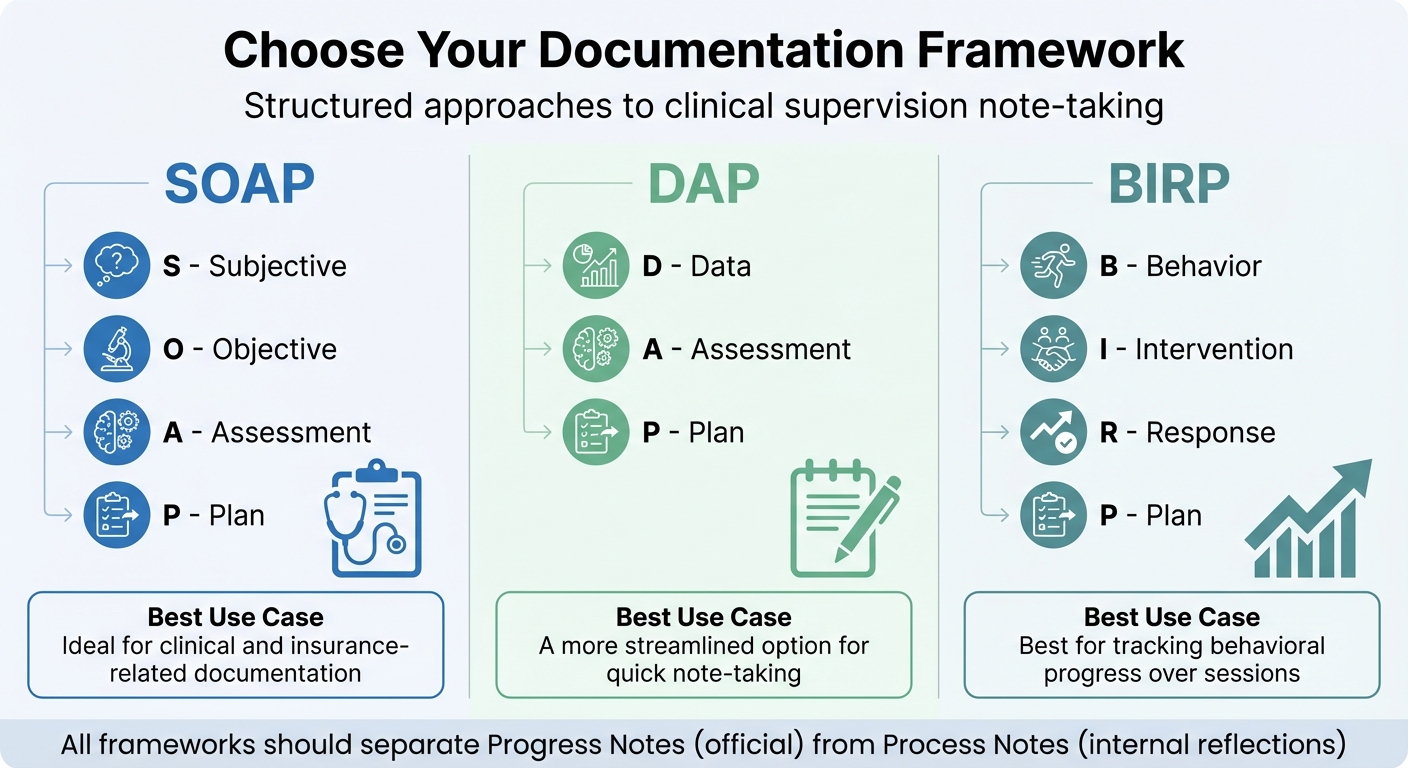
Using a consistent framework can make your notes clear and easy to reference. Popular formats include SOAP, DAP, and BIRP. These help organize information systematically and ensure nothing important is missed.
| Format | Components | Best Use Case |
|---|---|---|
| SOAP | Subjective, Objective, Assessment, Plan | Ideal for clinical and insurance-related documentation |
| DAP | Data, Assessment, Plan | A more streamlined option for quick note-taking |
| BIRP | Behavior, Intervention, Response, Plan | Best for tracking behavioral progress over sessions |
It’s important to separate Progress Notes (official clinical documentation) from Process Notes (your internal reflections). This distinction protects sensitive insights while maintaining a clear audit trail. Writing immediately after each session ensures accuracy and completeness. Once finalized, authenticate the notes and store them securely to complete the process.
Signatures and Secure Storage
Every note should be signed and dated by both the supervisor and supervisee. This dual signature approach confirms active participation and ensures traceability for licensing boards or legal reviews. For digital systems, timestamps on signatures add an extra layer of integrity.
As Angela M. Doel, Psychotherapist, puts it: "Appropriate documentation and supervision notes further underscore their commitment to transparency, accountability, and maintaining the highest ethical standards in their practice."
Store supervision records in a secure, encrypted system or a locked physical cabinet with restricted access. Ensure the storage method includes audit logs and regular backups to comply with HIPAA standards. Clarify who holds the legal responsibility for the records – whether it’s you, your agency, or your facility – to avoid confusion and prevent breaches down the line.
Best Practices for Supervision Documentation
Building on the foundation of session details and secure storage, these strategies can help streamline your documentation while ensuring compliance with licensing and legal standards.
Using Templates and Agendas
Standardized templates are a game-changer for supervision documentation. They provide a structured framework to record session objectives, interventions, and action items, making your notes consistent and efficient across supervisees and sessions.
A well-prepared agenda can also maximize your time. Focus on three key areas: 1) reviewing previous action items, 2) discussing client cases, and 3) addressing ethical or self-care concerns. This structure ensures that important topics are covered without wasting time.
As Anthony P. Onorato, MA, LPC, ALPS, AADC, says: "Details matter… they matter when we help people better understand themselves so they can live in a manner that is more meaningful and fulfilling to them. And they matter when we document our encounters."
To save even more time, consider using keyboard shortcuts for frequently used phrases. Once your template is in place, double-check that your records remain confidential.
Protecting Confidential Information
Confidentiality is critical. Instead of full names, use client initials or unique IDs to adhere to HIPAA standards. For remote sessions, document the HIPAA-compliant platform you used and confirm client consent.
Strengthen security on your devices by enabling multi-factor authentication (MFA), full-disk encryption, and remote-wipe capabilities in case of loss or theft. Role-based access controls can limit staff access to only the information they need. And avoid using public Wi-Fi for accessing electronic health records (EHR) or supervision notes – it’s a common weak spot for data breaches.
Here’s a sobering fact: human error is responsible for over 50% of healthcare data breaches, and the average cost of a breach in the U.S. is $7.42 million per incident. To avoid becoming a statistic, conduct security risk assessments every 1–2 years to uncover vulnerabilities. Also, review your EHR access logs monthly to spot unusual activity or unauthorized access.
By prioritizing data security, you create a solid foundation for consistent and timely documentation.
Documenting Sessions Consistently
Timeliness is key. Aim to document each session within 24 hours to ensure accuracy and readiness for audits. Delaying increases the risk of forgetting details or confusing sessions.
Before finalizing your notes, confirm they include essential details like the date (MM/DD/YYYY), start/stop times, modality, ethical challenges, risk assessments, and how interventions align with treatment goals.
To stay ahead of compliance issues, perform quarterly audits of your documentation. Missing data – such as mental status exams or risk assessments – can lead to serious consequences. For supervisees, failing to document the supervision-to-clinical-hours ratio could result in losing credit for up to 33% of their hours toward licensure. A proactive review process can help avoid these pitfalls and keep everyone on track.
Legal and Ethical Requirements
Supervision documentation isn’t just about staying organized – it’s a critical shield for both supervisees and the public. State licensing boards establish clear standards, and failing to meet them can jeopardize a supervisee’s path to licensure or expose supervisors to potential legal risks.
Meeting Licensing Board Requirements
Most states enforce specific ratios of clinical work to supervision hours. For instance, West Virginia mandates a 20:1 ratio, meaning supervisees need 1 hour of supervision for every 20 hours of direct client contact. Falling short of this can have serious consequences. If a supervisee works 30 hours a week but only receives 1 hour of supervision (a 30:1 ratio), they might only get credit for 20 hours toward licensure under such rules. That’s a significant loss – one-third of their hard-earned hours.
"Your ability to use the supervision hours is only as good as your ability to document the fact that you completed the supervision." – Brian Carnahan, Executive Director of the Ohio Counselor, Social Worker, and Marriage and Family Therapist Board
California’s Board of Behavioral Sciences is even more specific, requiring 3,000 hours of supervised experience over at least 104 weeks. Supervision agreements must be signed within 60 days of starting, and weekly logs must be signed every week. Similarly, the National Board for Certified Counselors (NBCC) mandates 100 hours of supervision alongside 3,000 hours of clinical work for national certification. Using incorrect forms or formats for documentation can invalidate hours entirely, so it’s crucial to verify your state’s requirements.
To stay compliant, maintain a formal supervision agreement, weekly logs, and periodic evaluations. Each record should detail the date, session length, format, topics discussed, and any necessary follow-up. These records are not just a formality – they’re your proof of adherence to the law and professional standards.
Recording Ethical Decisions
When ethical dilemmas arise – boundary concerns, conflicts of interest, or sensitive cultural issues – documenting your reasoning and feedback is essential. This creates a transparent record of your professional judgment.
As a supervisor, you act as a "gatekeeper." If you decide not to recommend a supervisee for independent licensure, your records must clearly show why. This includes detailed feedback, specific goals for improvement, and documentation of any lack of progress. For example, instead of vaguely stating, "supervisee showed poor judgment", write something concrete like, "supervisee did not consult with me before terminating client X despite our agreement to review all termination decisions."
By keeping your documentation factual and objective, you protect yourself and the supervisee from potential misunderstandings or legal disputes. Ethical and skill-based feedback should always be clear, actionable, and recorded consistently.
Consent and Privacy Documentation
The supervisory relationship begins with a written contract outlining expectations, responsibilities, and documentation practices. This agreement should cover everything from time commitments and client assignments to malpractice insurance and evaluation criteria.
Supervisees must give explicit consent to the supervision process, including how their performance and client cases will be documented and stored. If you’re using video-based supervision, ensure clients also provide consent at the start of treatment, and include this in their care plan. Only use HIPAA-compliant platforms like Zoom for Healthcare or Doxy.me to avoid privacy violations.
It’s also critical to define who controls the supervision records – whether it’s the supervisor, the agency, or the facility. This determines who has the legal authority to grant or deny access and ensures compliance with HIPAA regulations. While state rules vary, the general recommendation is to retain supervision records for at least 7 years, treating them with the same care as clinical patient records.
To safeguard these records, use locked electronic health records (EHR) systems or encrypted cloud storage with strict access controls and audit trails. Never delete original entries; instead, add timestamped corrections or addenda to preserve the audit trail. Proper documentation not only fulfills legal requirements but also supports professional development and accountability.
Using Voice CRM for Supervision Documentation
Meeting the strict documentation standards set by licensing boards doesn’t have to mean drowning in endless paperwork. Voice CRM simplifies the process with smart automation tailored for mental health professionals handling supervision requirements.
Voice-to-Text for Supervision Notes
Voice CRM takes the hassle out of documentation by using standardized templates and agendas to guide your process. With just one tap, supervisors can record session details immediately after they happen – capturing insights while they’re still fresh. Simply speak your observations, and AI-powered transcription will instantly create formatted notes. Forget about typing; this feature alone can save users over 10 hours a week on documentation tasks. Plus, the immediate transcription feature helps you meet the 24-hour standard for recording sessions.
The system automatically links transcribed notes to the correct supervisee’s record or supervision case, cutting out the need for manual filing. It also offers tools for supervision-specific tracking, allowing you to organize sessions by client discussions or broader professional development topics. This makes it easier to track a supervisee’s progress over time and quickly pull up specific sessions during licensing board reviews.
Organizing Notes with Thematic Tags
Thematic tagging turns your supervision notes into a powerful, searchable knowledge base. By applying tags like "boundary concerns" or "cultural competence", you can easily sort and review recurring ethical issues without wading through endless entries.
A hierarchical tagging system allows you to use broad categories alongside more specific sub-themes, keeping your growing database organized and easy to navigate. Even as your records expand, this system ensures everything stays accessible and clutter-free. These tools also integrate seamlessly with advanced security measures, offering a complete solution for documentation.
HIPAA-Compliant Security Features
Voice CRM ensures supervision records are secured with AES-256 encryption, safeguarding data both during transmission and while stored. The platform also provides a signed Business Associate Agreement (BAA) for HIPAA compliance and deletes audio recordings immediately after transcription, minimizing the risk of sensitive conversations lingering in cloud storage.
Role-based access controls restrict who can view supervision notes, while detailed audit logs track every action – from creating to editing notes. These features ensure only authorized users access records and provide a full audit trail for compliance checks.
Given that the average cost of a HIPAA violation reached $10.9 million per breach in IBM‘s 2023 Cost of Data Breach Report, these robust security measures are vital for protecting your practice and your supervisees’ future.
Conclusion
Thorough clinical supervision documentation is more than just a professional habit – it’s a safeguard for both supervisees and clients. Poor documentation can derail licensure progress and leave practices vulnerable to legal challenges. Thankfully, modern tools make it easier to meet these legal and ethical responsibilities.
Consistency is crucial. Aim to document sessions within 24 hours, use structured frameworks to organize your notes, and separate official progress notes from private process notes. Always store records in encrypted, HIPAA-compliant systems. As noted earlier, supervision records are typically retained for at least seven years to meet professional standards.
Voice CRM simplifies this process by taking the administrative load off your shoulders. Its voice-to-text transcription, thematic tagging, and AES-256 encryption ensure you can document quickly and securely. By combining speed with compliance, this platform allows you to focus on what matters most – your work with supervisees and clients.
Every detail counts when it comes to supervision documentation. Whether you’re tracking a supervisee’s development, passing a licensing board review, or protecting your practice from legal risks, maintaining accurate and organized records is essential. With the right tools and consistent habits, you can keep your documentation thorough and efficient, supporting both professional growth and client safety throughout the supervisory process.
FAQs
What counts as a supervision hour?
A supervision hour generally consists of documented, real-time interactions between a supervisee and a supervisor. These sessions can be one-on-one or involve a group, focusing on areas such as assessment, diagnosis, treatment planning, and ethical considerations. Proper records should detail the session date, duration, topics discussed, and both parties’ signatures to meet documentation requirements.
Who legally owns supervision notes at an agency?
Supervision notes typically belong to the agency that generates them. These records serve to fulfill the agency’s legal and ethical responsibilities, ensuring both compliance with regulations and accountability in practice. Keeping detailed and accurate documentation is a key part of maintaining professional standards.
How do I correct a supervision note without breaking compliance?
To address a supervision note while following compliance rules, never delete signed notes – doing so could violate legal and ethical guidelines. Instead, make a correction by adding a new entry. Clearly explain the adjustment, include the date, and sign the update. This approach keeps the record transparent, preserves its integrity, and ensures you remain within compliance standards.


